Reid Friesen DDS, MSc, FRCD(C); Dennis Chen BDSc (DH), DMD; Jonathan Chu BMSc, DDS; Tobias Mesizinger DMD, Maria Mushtaq BDS (Oral Medicine Graduate Program, Mike Petryk School of Dentistry, Faculty of Medicine & Dentistry, University of Alberta)
Oral cancer is uncommon in general dental practice, but missed diagnoses carry significant consequences. Survival remains strongly stage-dependent, and many cases are still identified late. For most patients, the first opportunity for detection occurs during routine dental care, placing general dentists in a critical position. The most impactful advances in detection are not technological, but clinical, occurring during routine examinations.
Rethinking Risk: Who Are We Screening?
Tobacco and alcohol remain important risk factors for oral cancer, particularly when used in combination. However, the epidemiology of head and neck malignancy has changed. HPV-associated cancers, particularly those arising in the oropharynx, are increasingly encountered and often occur in younger patients without traditional risk factors. In addition, oral cavity cancers may also arise in patients with no clearly identifiable risk profile.
A routine visual and tactile examination of the oral soft tissues should remain part of comprehensive dental care for all patients. This examination is appropriate for the detection of clinically evident lesions within the oral cavity. However, clinicians should recognize that it is not a reliable screening method for early HPV-associated oropharyngeal cancer, which often develops in sites not readily assessed on routine dental examination.
What Does an Effective Screening Exam Look Like?
A structured clinical examination remains the most practical and effective method for opportunistic screening in dental practice. A comprehensive examination should include:
- Extraoral assessment including cervical lymph nodes
- Systematic intraoral inspection
- Palpation of high-risk anatomical sites

Systematic extraoral assessment demonstrating palpation of the cervical lymph node chains.


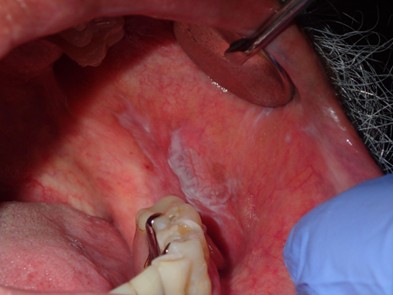
Assessment of a high-risk anatomical site, the lateral tongue, using gauze to facilitate retraction and improve visualization. Proper retraction allows for thorough inspection of areas where early lesions may otherwise be missed.
Intraoral and extraoral bimanual palpation technique used to assess the floor of mouth. This approach allows for detection of induration, masses, or submucosal changes not apparent on visual examination alone.
Particular attention should be given to:
- Lateral and ventral tongue
- Floor of mouth
- Soft palate and accessible oropharynx
Palpation is a critical but frequently underperformed component of the examination. Subtle induration, fixation, or submucosal changes may not be visually apparent and can be easily overlooked without a thorough tactile assessment.
Suspicious findings include:
- Ulcers persisting beyond 2 to 3 weeks
- Leukoplakia (white changes)
- Erythroplakia (red changes)
- Mixed red and white lesions
- Induration on palpation
- Unexplained bleeding
The objective of screening is not to establish a definitive diagnosis at chairside, but rather to identify abnormal tissue behavior and initiate appropriate and timely referral.


Oral Potentially Malignant Disorders: What Recent Evidence Shows
Oral potentially malignant disorders, OPMDs, remain one of the more challenging areas in practice. Recent systematic reviews continue to show that these lesions are biologically heterogeneous and cannot be reliably risk-stratified based on appearance alone (Pimenta-Barros, 2025).
Leukoplakia is common, but risk varies widely. Non-homogeneous lesions, lesions on the tongue or floor of mouth, and proliferative patterns carry higher malignant potential.
The key clinical message is consistent:
- Appearance alone is not enough
- Prolonged observation without biopsy can delay diagnosis
- Histopathology remains the gold standard
Persistent lesions require escalation, not indefinite monitoring.

Adjunctive Screening Tools
Adjunctive tools such as tissue autofluorescence devices, for example VELscope, chemiluminescence systems such as ViziLite, and vital staining with toluidine blue remain widely discussed in both clinical and commercial settings. Current evidence, however, supports a more measured view.
These tools may enhance visualization of mucosal abnormalities, but they do not reliably distinguish benign from dysplastic or malignant lesions, and false positives are common, particularly in the presence of inflammation or trauma (Lau, 2024).
Newer approaches, including oral cytology-based platforms, narrow-band imaging, and optical imaging technologies, show greater promise but remain largely within specialist or research settings and require further validation (Pierfelice, 2024).
In practice, adjunctive tools may support assessment, but they do not replace biopsy or appropriate referral when clinical suspicion exists.

What’s New: Where Screening is Heading
Several developments are shaping the future of oral cancer screening, although most remain in early stages of clinical adoption.
Salivary biomarkers continue to evolve, with emerging data suggesting improved diagnostic performance. At present, they are best viewed as adjuncts for risk stratification rather than definitive diagnostic tools (Khijmatgar, 2024).
Artificial intelligence is emerging in image-based screening and lesion triage. Early evidence suggests it may improve detection consistency and support decision-making, particularly in settings with limited specialist access, though it remains dependent on validation and image quality (Singh, 2025).
Other innovations, including advanced imaging and cytology-based techniques, aim to detect tissue changes not visible during routine examination, but are not yet widely used in general practice.
Overall, screening is moving toward multi-modal, non-invasive approaches. However, the clinical foundation remains unchanged: careful examination, appropriate suspicion, and timely biopsy or referral continue to define accurate diagnosis.
Biopsy and Referral: Acting Early Matters
Delayed referral remains one of the most preventable contributors to late-stage diagnosis. A simple approach:
- Lesions persisting beyond 2 to 3 weeks
- Lesions with concerning features
- Lesions that are changing or progressing
These should prompt biopsy or referral. Clinicians who choose to perform biopsy must also be equipped to coordinate appropriate follow-up and management, including ongoing care or referral for lesions such as leukoplakia.
Clinicians with expertise in oral mucosal disease, particularly specialists in oral medicine and pathology, as well as oral and maxillofacial surgeons, play a central role in diagnosis and management. Academic programs, including the Oral Medicine Graduate Program at the University of Alberta, serve as important referral resources for assessment and biopsy planning. The Oral Medicine Graduate Program is an important resource for patient care and also plays a key role in training future specialists in Alberta.
The key principle is timely action.
What Dentists Commonly Miss
This is where small changes in practice can have a large impact.
- Skipping palpation of the tongue and floor of mouth
- Assuming trauma without reassessment
- Monitoring lesions without a defined follow-up plan
- Relying too heavily on risk factors
- Being reassured by a “benign appearance”
- Delaying referral while waiting for resolution
A useful rule is simple. If a lesion does not look or behave like normal tissue, it deserves follow-up or escalation.
Documentation and Clinical Responsibility
Documentation supports both patient care and professional responsibility. Records should include:
Site and size
Clinical description
Duration and progression
Clinical decision
It is also important to document that a screening examination was performed, even when findings are normal.
Where feasible, high-quality clinical photographs are strongly recommended. Photography provides an objective baseline, supports monitoring of lesion progression over time, and can be invaluable when communicating with specialists or facilitating referral.
What Actually Changes Outcomes
- Despite ongoing innovation, the most meaningful improvements in detection still come from:
- Consistent examination
- Recognition of high-risk features
- Early referral
- Delays are more often related to clinical decision-making than lack of available tools (Lau, 2024). The fundamentals continue to matter most.
Take-Home Points for Daily Practice
- Perform a structured screening at every recall
- Do not rely on risk factors alone
- Palpate routinely
- Reassess any suspicious lesion beyond 2 to 3 weeks
- Use adjunctive tools cautiously
- Refer early
- Document clearly
References
- Lau M, et al. Adjunctive aids for the detection of oral squamous cell carcinoma and oral potentially malignant disorders, a systematic review of systematic reviews. Journal of Dental Sciences Review. 2024. https://doi.org/10.1016/j.jdsr.2023.12.004
- Pierfelice M, et al. The diagnostic potential of non-invasive tools for oral cancer and precancer, a systematic review. Diagnostics. 2024;14(18):2033. https://doi.org/10.3390/diagnostics14182033
- Khijmatgar S, et al. Salivary biomarkers for early detection of oral squamous cell carcinoma and head and neck squamous cell carcinoma, a systematic review and network meta-analysis. Journal of Dental Sciences Review. 2024. https://doi.org/10.1016/j.jdsr.2023.10.003
- Pimenta-Barros P, et al. Malignant transformation of oral leukoplakia, systematic review and comprehensive meta-analysis. Oral Diseases. 2025. https://doi.org/10.1111/odi.15140
- Singh V, et al. Screening tools and strategies for early detection of oral cancer and potentially malignant disorders in rural and low-resource populations, a systematic review. Journal of Oral and Maxillofacial Surgery. 2025. https://doi.org/10.1016/j.jormas.2025.102667